Macular pucker, also known as an epiretinal membrane or cellophane maculopathy, is a condition that affects the macula, a small area located in the center of the retina at the back of the eye. The macula is responsible for central vision, which allows us to see fine details and perform tasks such as reading, driving, and recognizing faces.
Causes of Macular Pucker
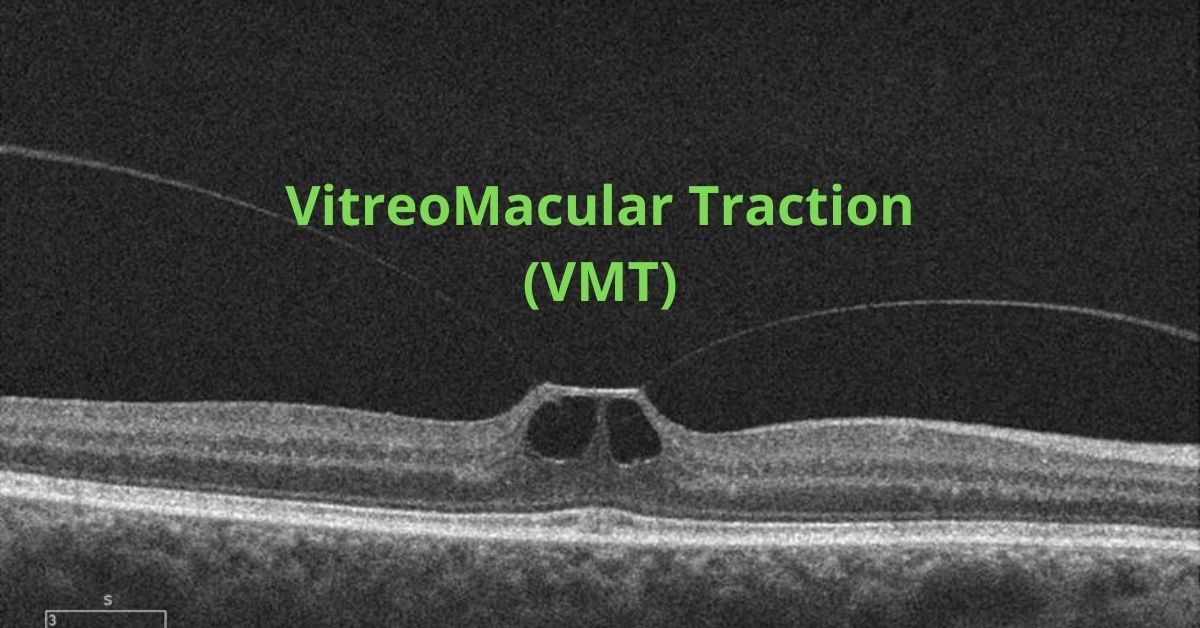
Macular pucker occurs when a thin, transparent layer of scar tissue forms on the surface of the macula. This scar tissue can cause the macula to wrinkle or pucker, leading to distorted and blurred vision. The most common cause of epiretinal membrane development is aging, as the vitreous gel inside the eye shrinks and pulls on the macula, causing the formation of scar tissue. However, other factors such as eye trauma, inflammation, and certain eye conditions can also contribute to its development.
Symptoms of Macular Pucker
Symptoms of macular pucker can vary from mild to severe and typically affect only one eye. Common symptoms include blurred or distorted central vision, difficulty reading or performing tasks that require good vision, and the appearance of straight lines as wavy or bent. In some cases, individuals may also experience a gray or cloudy area in their central vision.
While macular pucker can cause significant visual impairment, it can vary in severity. In mild cases, no treatment may be necessary, and individuals can adapt to their vision changes. However, in more severe cases where vision loss significantly affects daily activities, surgical intervention may be recommended.
Treatment Options
The most common surgical procedure for macular pucker is called vitrectomy with membrane peeling. During this procedure, the vitreous is removed from the eye and the scar tissue on the macula is carefully peeled away. Following surgery, visual recovery may take several weeks to months, but not all individuals will regain normal vision.
Regular eye examinations are important for the early detection of macular pucker or other eye conditions. If you experience any changes in your vision, I recommend you inform your own doctor to provide a proper diagnosis and recommend appropriate treatment options after examining you.
If you would like to schedule an appointment, please call us (877) 245.2020.