Vitreous hemorrhage from various causes can cause floaters.
Vitreous hemorrhage can cause floaters in the eye. Bleeding inside the eye is called vitreous hemorrhage. Symptoms of this type of bleeding range from a showere of floaters to incomplete darkness (lots of blood).
Floaters due to blood can not be distinguished by other types of floaters based upon appearance. Often floaters from hemorrhage have appeared suddenly and don’t necessarily last as long as chronic (long-lasting) floaters, but they can.
Causes of Vitreous Hemorrhage
Any bleeding into the vitreous is called vitreous hemorrhage. Hence, there are a variety of causes of bleeding into the vitreous;
- Retinal tears
- Retinal Detachments
- Trauma
- Diseases of the retina (eg. proliferative diabetic retinopathy)
- Complications of retinal vascular disorders
- Posterior Vitreous Detachment
Treatments
For all intents and purposes, blood in the vitreous does not cause long-lasting damage. It is most important to establish the underlying cause of the bleeding and treat that disorder whenever possible.
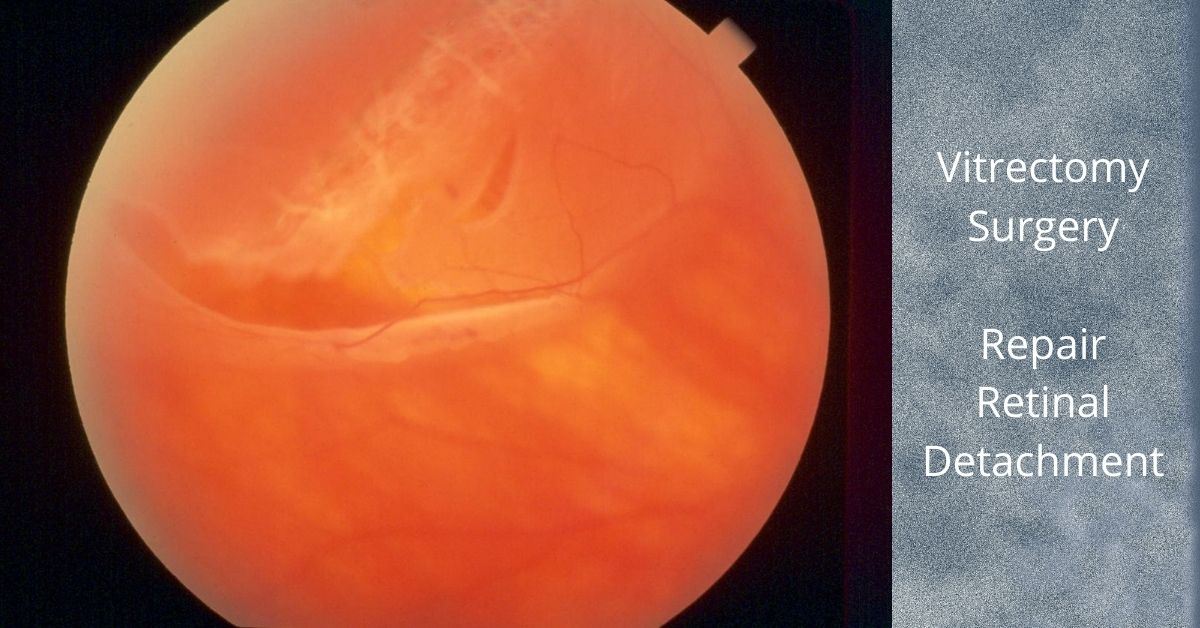
For dense vitreous hemorrhages, it may indeed be prudent to consider a vitrectomy to remove the blood to restore vision, but more importantly, and to allow the retina specialist to perform a thorough examination of the eye with the blood removed.
Retinal Tears and Bleeding
As an example, a retinal tear can cause a vitreous hemorrhage if the tear rips across a retinal blood vessel and causes bleeding. There may be too much blood to actually visualize a retinal tear. Keep in mind, retinal tears can lead to retinal detachments.
Retinal detachments can be potentially blinding and, in cases of all retinal tears, we would like to treat the tear before a retinal detachment develops.
Vitreous Hemorrhage Can Resolve
Blood in the vitreous usually absorbs and can clear on with a vitrectomy. There is no specific timing of this and it can take weeks or even months. Sometimes, blood does not clear on its own and vitrectomy may be necessary.
If you would like to schedule an appointment, please call us (877) 245.2020.