A Beovu study was halted recently.
In a May 28, 2021 press release, Novartis Pharmaceuticals halted an ongoing trial of BEOVU (brolucizumab) for the treatment of wet macular degeneration. About 1 year ago, there were concerns over Beovu and potential complications.
BEOVU, an anti-VEGF drug, is FDA approved for the treatment of wet macular degeneration and is delivered via intraocular injection. The approval also allows for the drug to be repeated as often as every 8 weeks. The trial was to determine if Beovu could be administered every 4 weeks instead of 8. Most of the other anti-VEGF medications can be given every 4 weeks.
Other anti-VEGF medications include:
- Lucentis (ranibizumab)
- Avastin (bevacizumab)
- Eylea (aflibercept)
All are given by intraocular injection and are powerful weapons for the treatment of macular degeneration, diabetic retinopathy and retinal vascular occlusions.
Why Study was Halted
This was originally a 2 year study where patients were treated every 4 weeks with Beovu. Great clinical studies are so-called “double blinded”, that is, neither patient nor treating physician knows what drugs are being delivered. This prevents bias in the study.
The results of the first year of the study were recently released which showed, when dosed at a higher frequency (4 weeks), an increase in the incidence of intraocular inflammation when compared to other studies.
The Beovu study was halted in the interests of patient safety. While most intraocular inflammation is well tolerated, that is, there is no long term sequalae, this conservative approach may save vision in many patients involved in the study as some patients may have permanently lost some vision.
This does not mean Beovu is not a good drug, it just means that studies indicate that the drug may have some toxicity if used too often. In the case of Beovu for macular degeneration, use every 4 weeks may be too often.
Presently the FDA has approved the drug to be used no more often than every 8 weeks.
Beovu Potential
Several studies have found that Beovu, when given only every 8 weeks, is a very potent and effective drug for wet macular degeneration, particularly in those patients where other drugs were unable to control the disease.
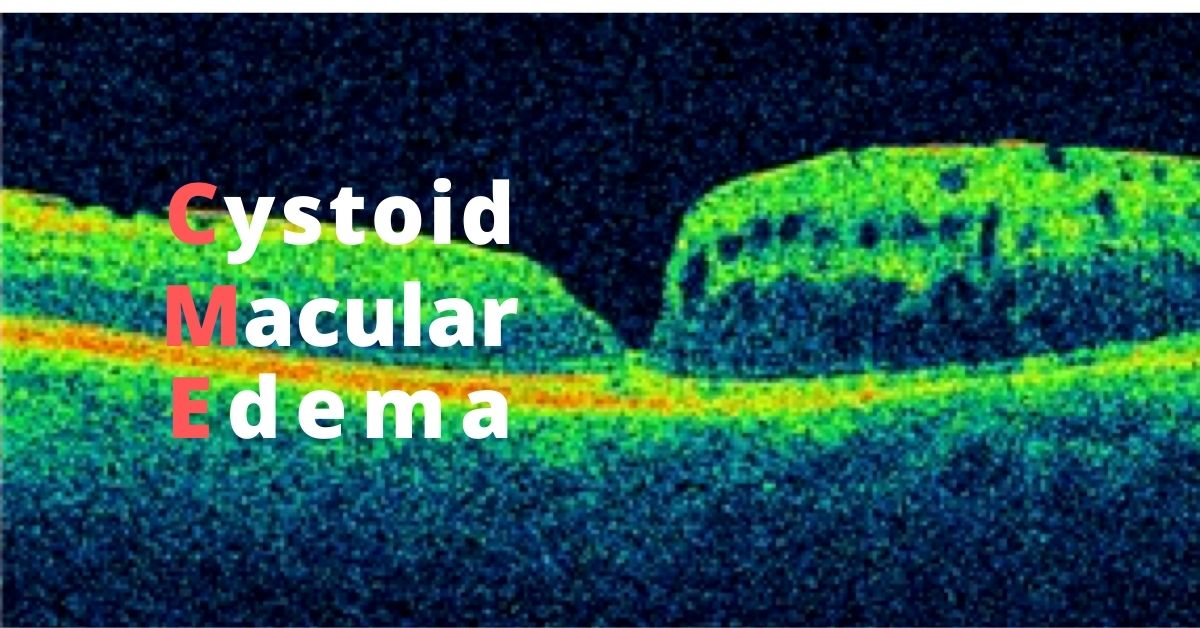
Ongoing clinical trials are testing the effectiveness of Beovu for treating diabetic macular edema (DME), a complication of diabetic retinopathy. Other anti-VEGF medications are also approved for the treatment of DME.
Retina specialists vary in their preference of anti-VEGF medications for certain conditions. Patient response to a particular medication often varies, for instance, consider the use of Tylenol, aspirin and ibuprofen. Though all can be used for pain relief, most of us find that one works better for us than the others.
It is very likely that Beovu will find it’s place in treating hard to treat patients with wet macular degeneration.
Stay tuned.
If you would like to schedule an appointment, please call us (877) 245.2020.